TAP Technology
Better, patient-centered results made easy with better tools.
Non-exercise cardiac stress testing in less time and with less risk of dysrhythmia as compared to dobutamine.
Radionuclide or echocardiography exams that would be difficult with conventional exercise testing.
Differential diagnosis of complex arrhythmias with amplified P-wave of the esophageal ECG.
Induction of SVT or flutter to evaluate atrial vulnerability or efficacy of anti-arrhythmia therapies (drugs, ablation).
Anti-tachycardia ("overdrive") pacing for cardioversion of supraventricular tachycardia (SVT) or atrial flutter.
Temporary atrial pacing for patients with bradycardia, hypotension or sick sinus syndrome (SSS).
Esophageal electrophysiology and temporary atrial pacing in infants and children with a 5 French catheter (TAPCATH).
Clinical Indications
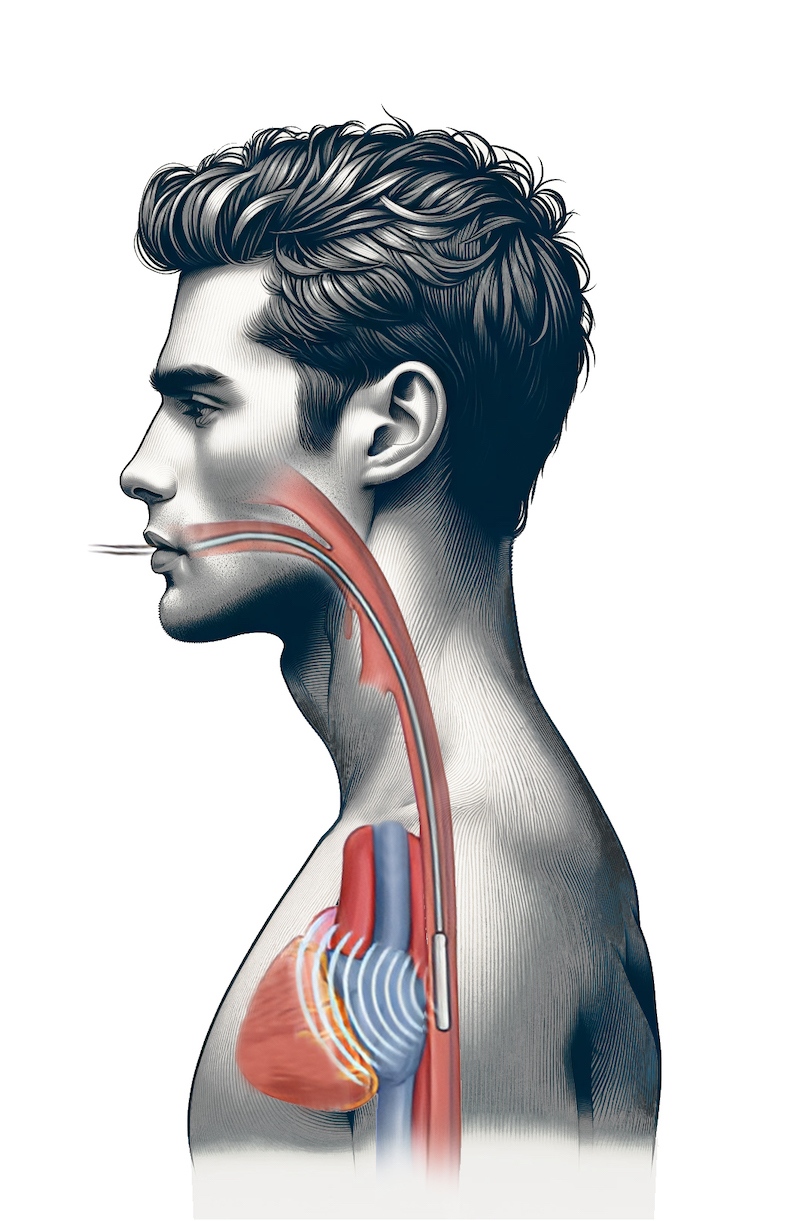
Our patented transesophageal technology puts you right next to the heart with a revolutionary noninvasive solution that delivers unprecedented temporary heart rate control.
Scientifically validated in over 250 clinical studies and in routine daily use in many U.S. hospitals, this breakthrough technology is changing medicine as we know it. For the anesthesiologist, heart rate and blood pressure now can be restored almost immediately, without drugs and worrisome side effects. For the cardiologist, non-exercise stress echocardiography tests can be conducted in half the time as compared to dobutamine stress echo, in the convenience of the cardiologist’s office. And electrophysiology studies show that transesophageal pacing can be used to both induce and terminate many SVTs in pediatric and adult patients, avoiding anesthesia and more invasive procedures.
And temporary atrial pacing is only the beginning. In fact, studies show that CardioCommand’s esophageal ECG can play an important role in the noninvasive diagnosis of abnormal left atrial electrical activity, useful for safely identifying patients for ablation of focal atrial fibrillation.
Far more than a new alternative, this is safer, faster and more cost-effective care . . . precisely what caregivers need to optimized outcomes in the face of the rising incidence of heart disease and related chronic conditions.
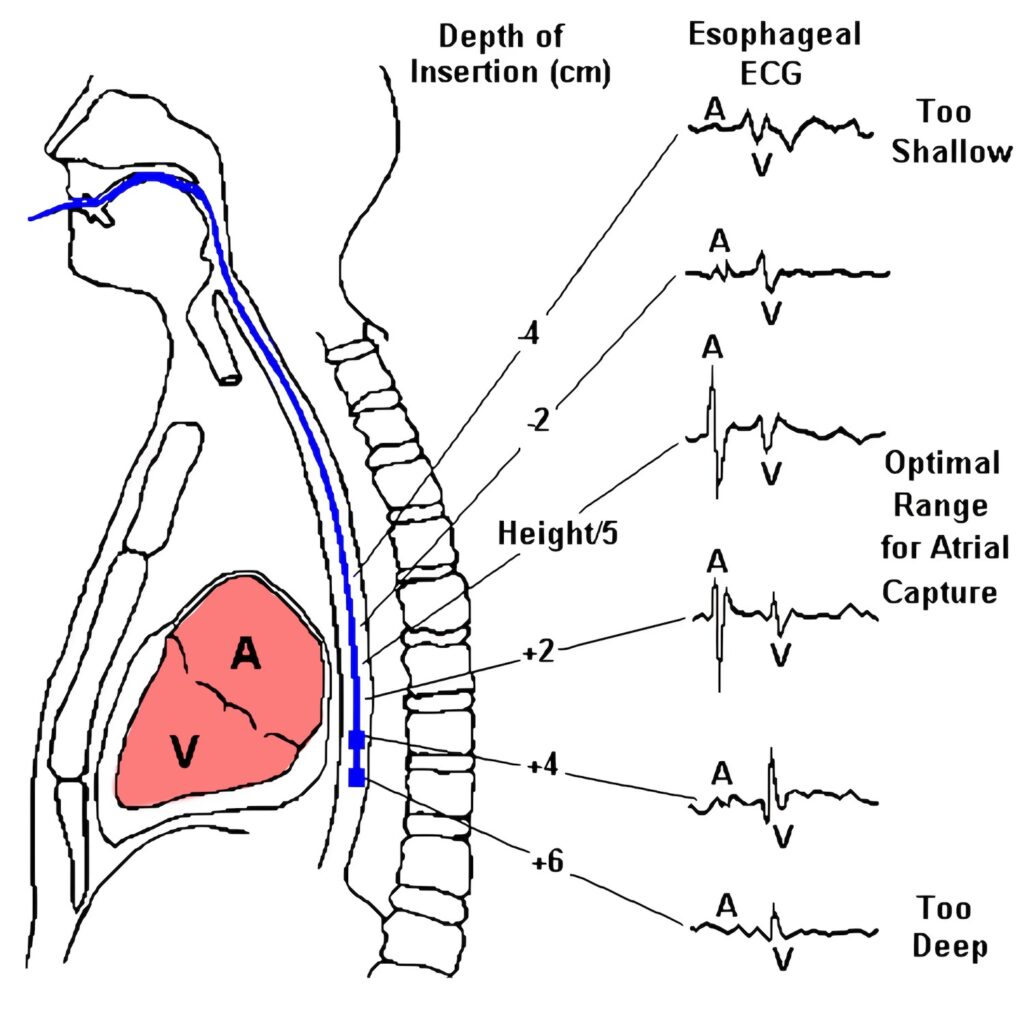
Optimal Positioning of Electrodes for Transesophageal Atrial Pacing
Using ECG tracings
Insert electrodes to an initial DOI = height/5 + 5 (for nasal: height/5 + 9 ) cm. While monitoring esophageal electrocardiogram, gradually withdraw catheter to the DOI which maximizes amplitude of the ECG P-wave (see below). Abstract
Using patient's height
Depth of insertion (DOI, cm) within the esophagus is printed on CardioCommand catheters. For oral insertion, the optimal range of DOI for atrial pacing can be estimated using patient height: DOI = height (cm) / 5, or height (ins) / 2. An additional 3 to 4 cm DOI should be used for nasal insertions. For most patients, atrial capture can be achieved within a range of +/- 3 cm about this DOI. For infants and children, it is recommended that electrodes be positioned with monitoring of the esophageal ECG. Abstract